
Addressing the Coding Variance That Impacts Practice Revenue
When we review a month-end report and see a spike in denials, the natural instinct is to look for a single person to blame. However, coding errors are rarely the result of a single oversight.
Instead, they are usually a symptom of a breakdown in communication between the clinical team and the billing department.
While some mistakes are obvious data entry errors, the most significant revenue impact often comes from “coding variance”, the subtle gaps in specificity or documentation that cause a claim to deviate from a payer’s requirements.
These errors result in a steady accumulation of unrealized revenue and administrative friction.
Capturing the revenue your practice has earned requires a system that identifies these patterns before they become systemic.
We will move past generic advice to look at the specific ICD-10 and CPT mistakes that cause operational delays and how to build a feedback loop that prevents them from recurring.
The Financial Impact of Coding Variance
It is important to understand the actual cost of a coding error beyond the missed payment. When a claim is rejected, it triggers a chain of events that increases your practice’s overhead.
According to industry benchmarks, the administrative cost to research, correct, and resubmit a denied claim can exceed $25.
If your team is managing dozens of these rejections every week, that labor cost adds up quickly. Every day a claim sits in “denied” status is a day your accounts receivable (AR) continues to age, which decreases the likelihood of full recovery.
The goal of a high-functioning revenue cycle is not to reach 100% perfection, which is nearly impossible given the complexity of payer rules, but to reduce the “cost to collect.”
By identifying coding patterns that lead to rejections, we can lower the administrative burden on your staff and stabilize your cash flow.
Precision Issues in ICD-10 Reporting
The ICD-10 system requires a level of diagnostic detail that demands constant attention.
With over 70,000 codes available, selecting the most accurate one is as much an operational challenge as a technical one.
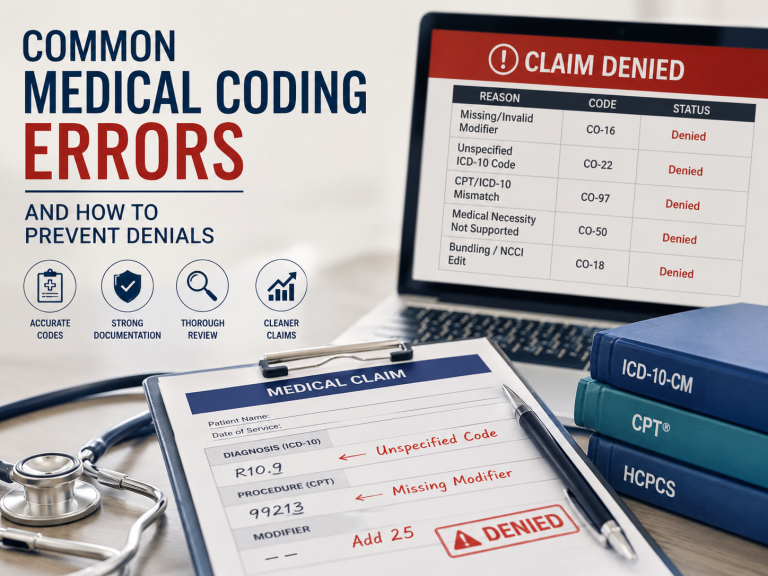
The Cost of “Unspecified” Codes
Payers frequently use automated logic to flag claims that use “unspecified” codes when more detailed options are available in the clinical record.
For example, selecting a general code for hypertension when the patient’s chart notes a more complex hypertensive crisis can lead to a denial for lack of medical necessity.
This often happens because a coder is working from a simplified list or a template that defaults to the easiest option. We recommend reviewing your most frequently used codes to make sure they allow for the level of specificity that payers currently require.
Managing Annual Code Updates
The Centers for Medicare & Medicaid Services (CMS) updates the ICD-10 code set every October.
If a practice fails to update its EHR templates or billing software, it will inevitably submit deleted or revised codes.
These are preventable rejections that stem from a technical oversight rather than a clinical one. Maintaining an updated code library is a basic but essential part of revenue stability.
CPT Accuracy and the Risk of Undercoding
While diagnosis codes explain the “why,” CPT codes explain the “what.” In many practices, the focus is often on avoiding overcoding to prevent audits, which often leads to the opposite problem: undercoding.
The Impact of Undercoding on Revenue
Undercoding occurs when a provider bills for a lower level of service than what they actually performed.
If you consistently document and deliver a Level 4 E/M service but bill at Level 3 out of “caution,” you are leaving earned revenue on the table.
Accurate coding is not about being aggressive; it is about reflecting the true complexity of the care provided. If the documentation supports the service, the practice should be reimbursed for it.
Unbundling and NCCI Edits
Unbundling happens when separate codes are used for parts of a procedure that should be submitted as a single bundled code.
Payers use National Correct Coding Initiative (NCCI) edits to catch these mismatches. While usually unintentional, repeated unbundling can be viewed as an audit risk. Understanding which procedures are bundled ensures that your submissions align with payer logic from the start.
Resolving the Documentation-to-Billing Gap
We find that most coding errors originate in the clinical note, not the billing office.
If a physician’s documentation is missing key details, the coder cannot legally select the most appropriate code. This creates a “documentation gap” that is often the root cause of repeated denials.
Instead of treating coding as a back-office task that happens after patient care, we should view it as a continuous feedback loop.
When a claim is denied because of a documentation issue, that information needs to flow back to the physician. This allows the clinician to see exactly how their notes impact the billing outcome and encourages more precise documentation habits in the future.
Building a Feedback Loop for Revenue Stability
To reduce the frequency of errors, a practice needs a proactive strategy. We recommend the following operational steps:
- Monthly Internal Reviews: Audit a random sample of claims against the original clinical notes. This helps you catch specificity gaps before they become a trend.
- Payer-Specific Denial Tracking: Some insurance companies have unique rules for certain codes. Tracking these specific requirements allows your team to adjust their submission habits accordingly.
- Pre-Submission Scrubbing: Utilize automated software or manual review to catch missing modifiers or mismatched codes before the claim is sent.
- Targeted Physician Education: Share specific examples of denied claims with the clinical team to show how small changes in documentation can prevent administrative delays.
Common Questions Regarding Coding Precision
1. How do “modifiers” affect my coding accuracy?
Modifiers (like 25 or 59) provide extra information about a service. When used correctly, they prevent unnecessary denials for “duplicate” services.
However, they are often scrutinized by payers. We recommend using them only when the documentation clearly shows that a service was distinct and separately identifiable.
2. Can our EHR templates lead to coding errors?
Yes. Many templates use pre-filled language that may not change from patient to patient.
If a template defaults to a general diagnosis code, the claim may lack the specificity required for payment. It is important to review your templates regularly to ensure they support accurate, encounter-specific documentation.
3. Why does “Medical Necessity” cause so many denials?
Medical necessity is the payer’s way of asking if a procedure was justified by the diagnosis. If your CPT and ICD-10 codes do not link logically, the claim will be denied.
This often happens if a coder selects the first diagnosis they see rather than the one that specifically justifies the procedure performed.
4. What is the difference between a “rejected” and a “denied” claim?
A rejected claim has a formatting error (like a missing NPI) and never enters the payer’s processing system. These can usually be fixed quickly.
A denied claim has been processed and found unpayable due to coding or policy issues. Denials are more expensive to fix because they require deeper research and an appeal.
5. Is it better to handle coding in-house or with a partner?
The right choice depends on your volume and staff expertise.
In-house coding offers direct control, but maintaining accuracy can be difficult when volume is high or staff members leave. An outsourced partner can provide access to certified coders who specialize in your field, which often leads to more consistent results and lower denial rates.
Strengthening Your Billing Performance
Reducing coding errors is not about achieving perfect results; it is about consistently applying operational standards.
When your documentation is precise and your billing team has a clear feedback loop with the clinicians, your revenue cycle becomes more predictable and less prone to friction.
At Nsight Global, we focus on the specific mechanics of your revenue.
We support practices by reviewing denial trends, identifying documentation gaps, and providing the medical billing services needed to maintain high submission standards.
Our end-to-end RCM services are designed to give you the clarity and support needed to resolve complex coding challenges.
If you would like a detailed look at your current denial patterns or want to discuss how to tighten your follow-up workflows, we are ready to assist.
Reach out to the Nsight Global team to find out how we can help you build a more reliable billing process.